The Consent That Wasn’t Given — And Perhaps Never Fully Can Be
There is a moment in medicine we rarely question.
A patient signs a form. A doctor proceeds. And we call it informed consent.
We have built an entire legal and ethical architecture around this moment. We treat it as the threshold between lawful treatment and violation. Between care and harm. Between the procedure a patient chose and the one that was done to them.
But what if the moment itself is a fiction we have all agreed to maintain? What if the signature we have placed at the centre of this framework was never really doing the work we needed it to do?
A Signature Is Not the Same as Understanding
In 2008, a woman walked into a hospital expecting a diagnostic procedure.
She had been experiencing prolonged, irregular bleeding. Her gynaecologist recommended a diagnostic laparoscopy — a keyhole procedure, minimally invasive, intended to look and assess. She consented to that. She understood that. She signed the form for exactly that.
She went under anaesthesia.
What followed was not a diagnostic procedure.
While she was unconscious, her surgeon identified endometriosis and proceeded — without waking her, without asking, without a second consent — to perform a hysterectomy and bilateral salpingo-oophorectomy. The removal of her uterus, both ovaries, and both fallopian tubes.
She woke up irreversibly altered. Surgically menopausal. Permanently infertile.
She had signed a form. She had not agreed to this.
That case — Samira Kohli v Dr. Prabha Manchanda — forced Indian medicine to confront something deeply uncomfortable: consent had been taken, but it had not been given.
The Supreme Court of India did not merely rule in her favour. It articulated something the system had been quietly avoiding: that consent must be real, not assumed. That a signature on a general consent form does not function as a blank authorisation for whatever a clinician encounters under anaesthesia. That a patient rendered unconscious retains rights — and that those rights do not transfer to the surgeon’s discretion simply because the patient is no longer in a position to exercise them.
The distinction sounds subtle. It is not.
One is an administrative act. The other is a human one.
And for decades, medicine had been perfecting the administrative act while the human one quietly atrophied.
The Comfort of Bolam
To understand why, you have to go back further.
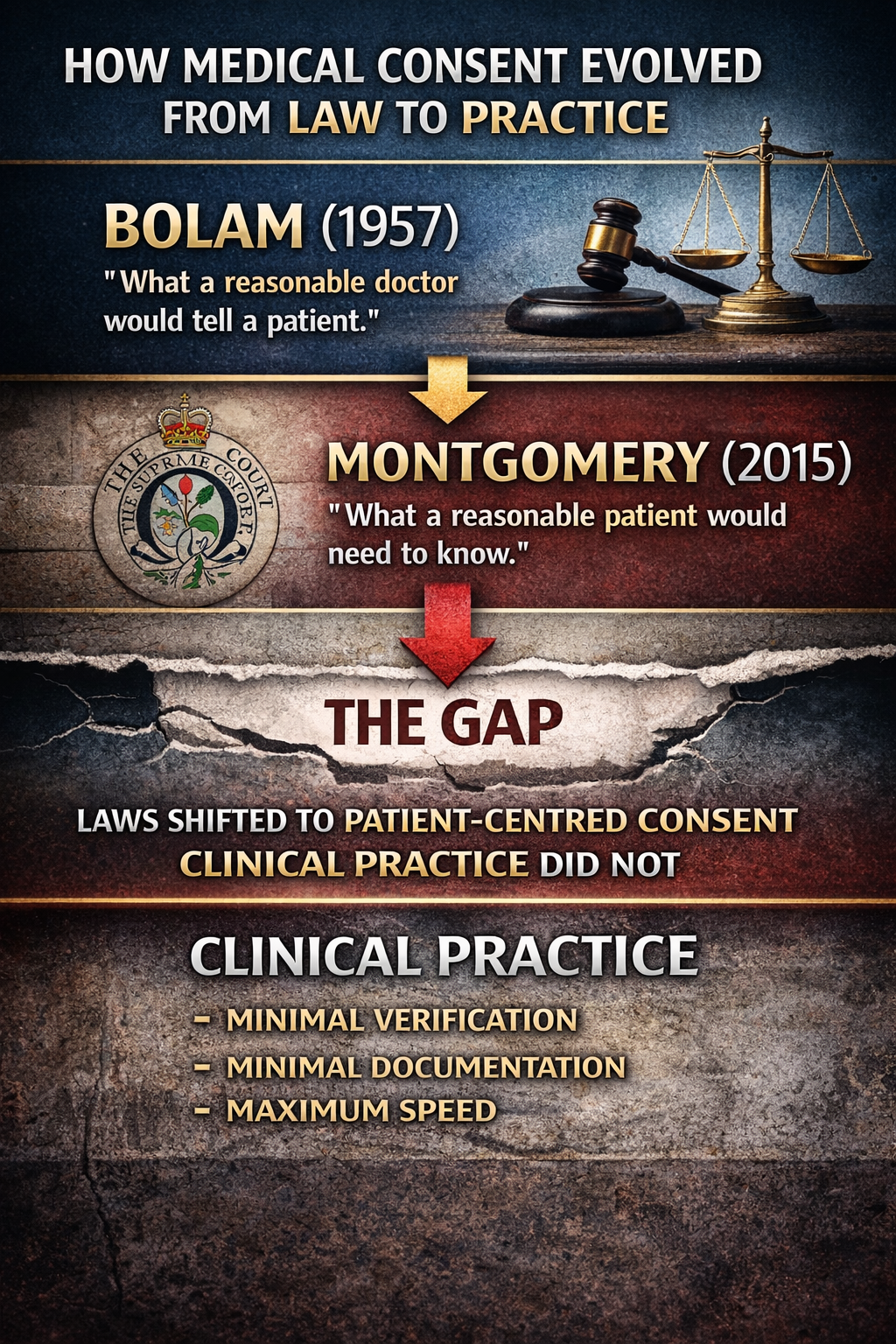
For much of the 20th century, medicine operated under the reassuring shelter of Bolam v Friern Hospital Management Committee (1957). The case arose from a patient who suffered fractures during electroconvulsive therapy — a procedure administered without muscle relaxants, and without a full explanation of the risks involved. The court’s response was to establish a principle that would govern medical negligence for decades: a clinician was not negligent if they acted in accordance with a practice accepted by a responsible body of medical opinion.
The principle was clean, collegial, and professionally convenient. If your peers would have done the same thing, you were protected. Medical standards were, in effect, set by the medical profession itself.
There is a logic to this. Medicine is complex. Judges are not clinicians. Deferring to professional consensus has a certain humility to it.
But Bolam carried a quiet assumption that would take decades to fully interrogate — that the clinician’s judgment about what a patient needed to know was sufficient. That disclosure was a professional act, calibrated by professional norms, evaluated by professional peers.
The patient’s understanding was, at best, a secondary consideration. At worst, it was simply not the point.
It was a framework built entirely on professional consensus. And it quietly ignored a deeper question — not whether the doctor had behaved as doctors do, but whether the patient had actually understood.
Those are not the same question. And for too long, medicine had allowed the first to stand in for the second.
When the Courts Began to Listen Differently
The correction, when it came, was gradual — and then, suddenly, decisive.
Chester v Afshar (2004) was an early signal that something was shifting. A neurosurgeon failed to warn his patient of a small but serious risk of paralysis associated with spinal surgery. The risk materialised. The patient was left disabled. The surgeon’s defence was straightforward: even if she had been warned, she would probably have had the surgery eventually anyway. The harm, in other words, was not caused by the failure to warn.
The House of Lords rejected that argument — and in doing so, fundamentally rethought the relationship between disclosure and causation. The patient’s right to be warned was not merely procedural. It was substantive. Failing to warn of a risk that then occurred was actionable, even when the counterfactual was uncertain. The law, in Chester, began to take seriously the idea that the opportunity to decide differently had its own value.
Then came Montgomery v Lanarkshire Health Board (2015) — the ruling that, in many ways, changed everything.
Nadine Montgomery was a diabetic woman of small stature carrying a large baby. Her obstetrician was aware of a significant risk of shoulder dystocia during vaginal delivery — a potentially catastrophic complication — but chose not to raise it, fearing the patient would opt for a caesarean section if informed. The birth proceeded. The shoulder dystocia occurred. The baby was deprived of oxygen for several minutes and suffered serious brain damage.
The UK Supreme Court set Bolam aside as the governing standard for consent and disclosure. In its place, it established a patient-centred test: a clinician must disclose any risk that a reasonable person in the patient’s position would consider significant. Not what the medical profession collectively deems appropriate to share — but what this patient, in this situation, would need to know to make a genuinely informed decision.
The clinician’s judgment about what a patient needs to know is no longer sufficient on its own.
Montgomery did not merely shift legal liability. It shifted the entire moral architecture of consent. It said, plainly, that patients are not passive recipients of clinical decisions. They are autonomous agents. And the role of the clinician is not to manage what the patient knows — it is to ensure the patient has what they need to decide.
Consent, at last in law, had become patient-centred.
At least, in theory.
The Uncomfortable Reality That Followed
Because here is where the story becomes genuinely difficult.
The law had arrived, through decades of litigation and refinement, at a standard that ethics had always pointed toward. Patient-centred. Autonomy-respecting. Disclosure of what a reasonable patient would consider significant.
And yet the operational reality inside most healthcare systems — including those formally bound by these very standards — has not kept pace.
Even today, in well-meaning, ethical, conscientious clinical practice, consent often looks like this: a form handed over in a pre-operative room, minutes before a procedure, by a clinician already mentally in the theatre. Pages of dense language that a health-literate person would struggle with, let alone a frightened patient encountering medical terminology for the first time. Risks disclosed in the passive voice, softened by clinical reassurance, shaped by the unspoken hope that the patient will simply agree and not complicate things further.
And underneath all of this, a set of forces that no form was ever designed to address.
Fear distorts cognition. A patient who has just received a serious diagnosis is not processing information the way they would in an ordinary conversation. Urgency compresses time. The power asymmetry between a patient in a hospital gown and a surgeon with thirty years of experience is not dissolved by a sheet of paper. And trust — the very thing that makes medicine function — can, in the wrong hands, become a mechanism of compliance rather than genuine agreement.
There is also something even more fundamental. Medicine itself is uncertain. Outcomes cannot be guaranteed. Risks cannot always be precisely quantified. The honest answer to many of the questions a patient most needs answered is, genuinely, we don’t know.
And you cannot fully inform someone about what is not fully known.
The Paradox at the Heart of Consent
Which is where we arrive at something uncomfortable.
We have constructed an entire legal and ethical framework on the premise of informed consent — in a system where information is genuinely complex, time is genuinely scarce, the relationship between clinician and patient is genuinely unequal, and outcomes are genuinely uncertain.
We demand a standard the system was never designed to meet. And then we use a signature as evidence that it was met.
It is worth asking, honestly: was informed consent ever meant to be perfect? Or was it always meant to be good enough — defensible enough — to allow medicine to proceed with some degree of moral legitimacy?
The tragedy of cases like Samira Kohli is not simply that consent failed. It is that the system had allowed itself to believe it had succeeded. The form was signed. The threshold, as the system understood it, had been crossed. That the patient woke up to a body she had not agreed to surrender was, within the logic of the system, an outcome rather than a violation.
That is the fiction. And it is one we have been maintaining, in courtrooms and operating theatres and pre-operative rooms, for a very long time.
The Gap Between What the Law Demands and What the System Delivers
Today, the law demands disclosure. Alternatives. Material risks. Evidence of genuine understanding. A patient-centred process, documented and defensible.
The system still largely delivers forms, speed, and signatures.
That gap is not a gap of intention. Most clinicians want to do this well. They entered medicine because they care about people, and the idea that a patient might feel violated by an experience they were supposed to have consented to is genuinely distressing to most of them.
It is a gap of design. Of infrastructure. Of a system that has evolved its legal obligations without building the tools, the time, or the processes to meet them. Clinicians are now held to a patient-centred standard of disclosure that their institutions have never equipped them to deliver. The law has moved. The system has not.
And patients remain caught in between — signing forms that satisfy an administrative requirement while the human act of genuine, comprehended, freely-given consent remains, in too many cases, aspirational.
Where This Leaves Us
Perhaps the real problem is not that consent is broken.
It is that we have been trying to solve a fundamentally human communication problem with a legal document. That we have confused the record of a conversation with the conversation itself. That somewhere in the journey from ethics to law to administration, the patient — the person whose body, whose life, whose consequences are actually at stake — became the last variable the system was designed around.
If we were to redesign consent honestly — from first principles, with everything we now know about communication, cognition, health literacy, shared decision-making, and the psychology of high-stakes choices — we would not start with a form.
We would start with a question.
What does this patient need to truly understand — not just to agree, but to decide?
And then we would build backwards from that. The conversation before the paperwork. The comprehension before the signature. The patient’s values and fears and questions treated as clinical information, not administrative inconvenience.
Because in the end, consent is not about protection. Not primarily. Not of the doctor, not of the hospital, not of anyone whose interests are served by a signed form on file.
It is about something older and more important than liability.
It is about a patient’s right to live with the consequences of a decision they actually made — fully, freely, and with their eyes open.
That is what informed consent was always supposed to be.
We are still — after Bolam, after Samira Kohli, after Montgomery, after all of it — working out how to make it so.
Shishir writes at Isaychaps.com — at the intersection of medicine, law, and the decisions that shape both.

You May Also Like
